If you use a CPAP machine, you’ve probably been told to focus on one number above all else: AHI (Apnea–Hypopnea Index). An AHI below 5 is often labeled a success. But many CPAP users know a frustrating truth:
You can have a “perfect” AHI and still wake up tired, foggy, or unrefreshed.
AHI is important—but it’s not the whole story. In this article, we’ll break down what AHI actually measures, what it misses, and which additional signals matter if your goal is restorative sleep, not just good-looking numbers.
What AHI Really Measures (and What It Doesn’t)
AHI counts how many apneas (breathing stops) and hypopneas (partial reductions in breathing) occur per hour of sleep.
It answers one narrow question:
How often did airflow drop below a defined threshold?
What it doesn’t measure:
- How hard your body worked to breathe
- Whether your sleep was fragmented
- How often your nervous system was activated
- Whether airflow was restricted but not reduced enough to count
AHI is a coarse metric—useful, but incomplete.
The Hidden Sleep Disruptors CPAP Users Often Miss
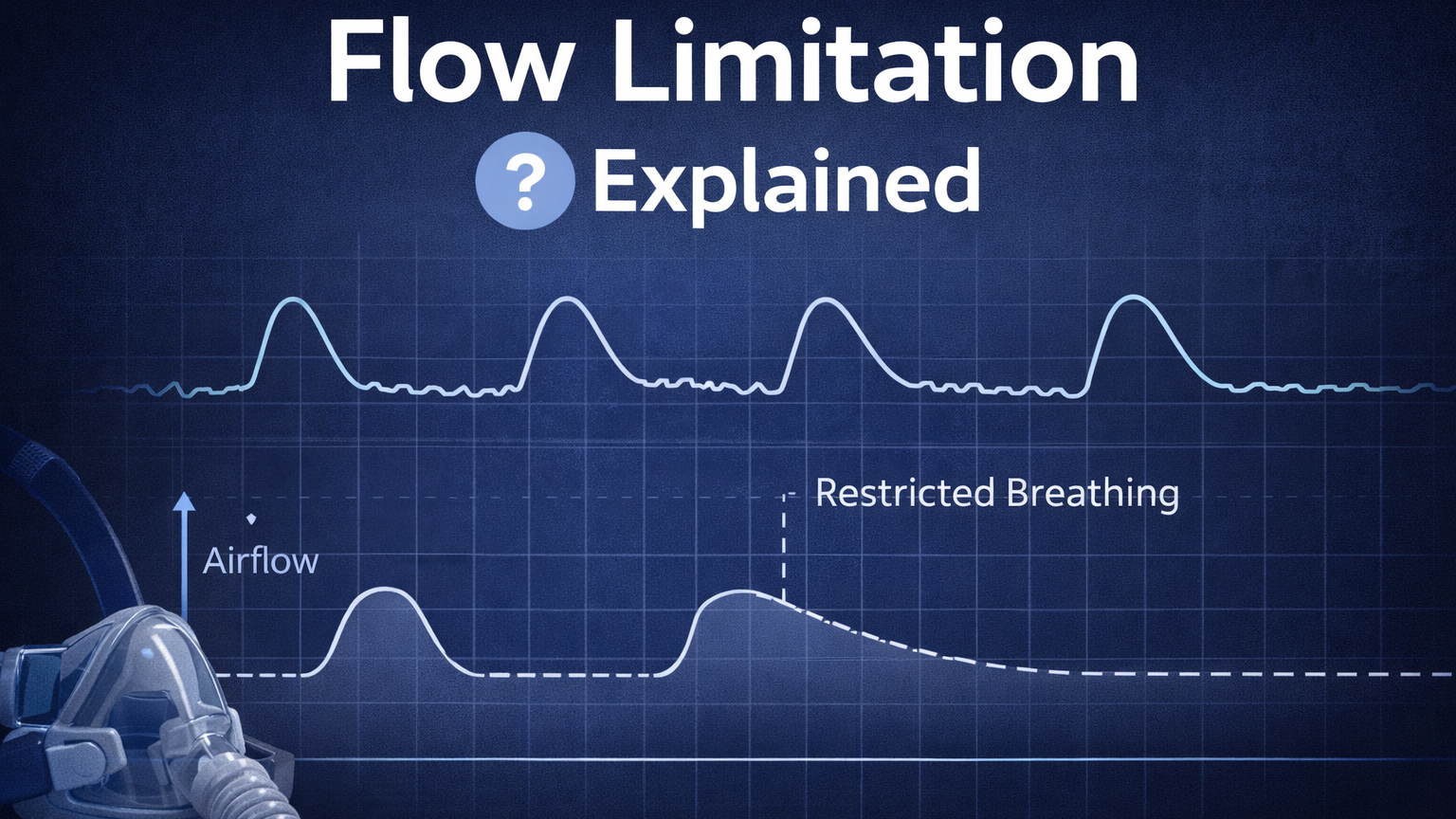
1. Flow Limitation: Breathing That’s Technically “Normal” but Not Healthy
Flow limitation occurs when your airway narrows just enough to restrict airflow—but not enough to trigger an apnea or hypopnea.
Effects can include:
- Increased breathing effort
- Micro-arousals from sleep
- Elevated heart rate and stress response
These events often don’t count toward AHI, yet they can severely degrade sleep quality.
2. RERAs and UARS: When Your Brain Keeps Waking You Up
RERAs (Respiratory Effort–Related Arousals) and UARS (Upper Airway Resistance Syndrome) involve repeated arousals caused by breathing effort—not airflow collapse.
Key issue:
- Sleep becomes fragmented
- Deep and REM sleep are reduced
- You wake up feeling exhausted despite “good” CPAP numbers
Many CPAP devices don’t clearly surface these events—or users don’t know where to look.
3. Sleep Fragmentation Matters More Than You Think
Your brain needs continuous, stable sleep to recover.
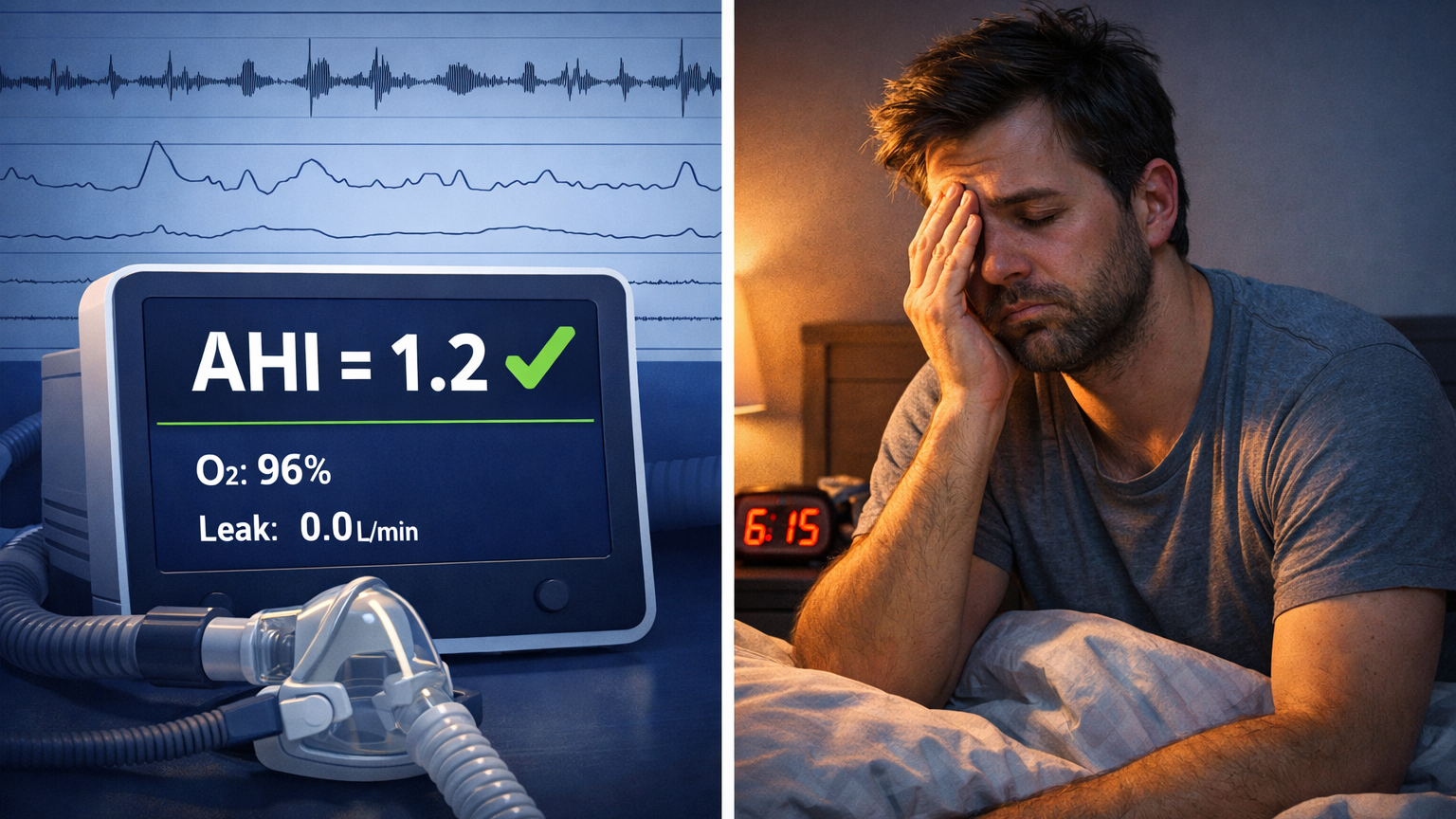
You can have:
- AHI = 1.2
- Zero large apneas
…and still experience:
- Dozens of micro-arousals
- Repeated transitions out of deep sleep
- Poor cognitive and physical recovery
AHI doesn’t reflect sleep continuity.
4. Oxygen Stability vs. Event Counts
Two people can have the same AHI—but very different oxygen profiles.
What matters:
- Depth of oxygen drops
- Duration of desaturation
- Frequency of recovery spikes
Short, frequent drops may never raise AHI significantly, yet still strain the cardiovascular system.
5. Pressure Comfort and Breathing Synchrony
Even when pressure is technically effective, issues like:
- Poor pressure transitions
- Inadequate EPR / pressure relief
- Mask resistance or leaks
can cause subtle breathing discomfort that repeatedly disrupts sleep—without increasing AHI.
Why “Chasing a Lower AHI” Can Backfire
Many CPAP users respond to lingering fatigue by:
- Increasing minimum pressure
- Disabling comfort features
- Narrowing pressure ranges aggressively
Sometimes this lowers AHI—but worsens sleep quality by:
- Increasing arousals
- Causing pressure-induced awakenings
- Disrupting natural breathing patterns
Optimization is about balance, not just suppression.
What You Should Look at Instead (or in Addition)
To truly understand your therapy, consider:
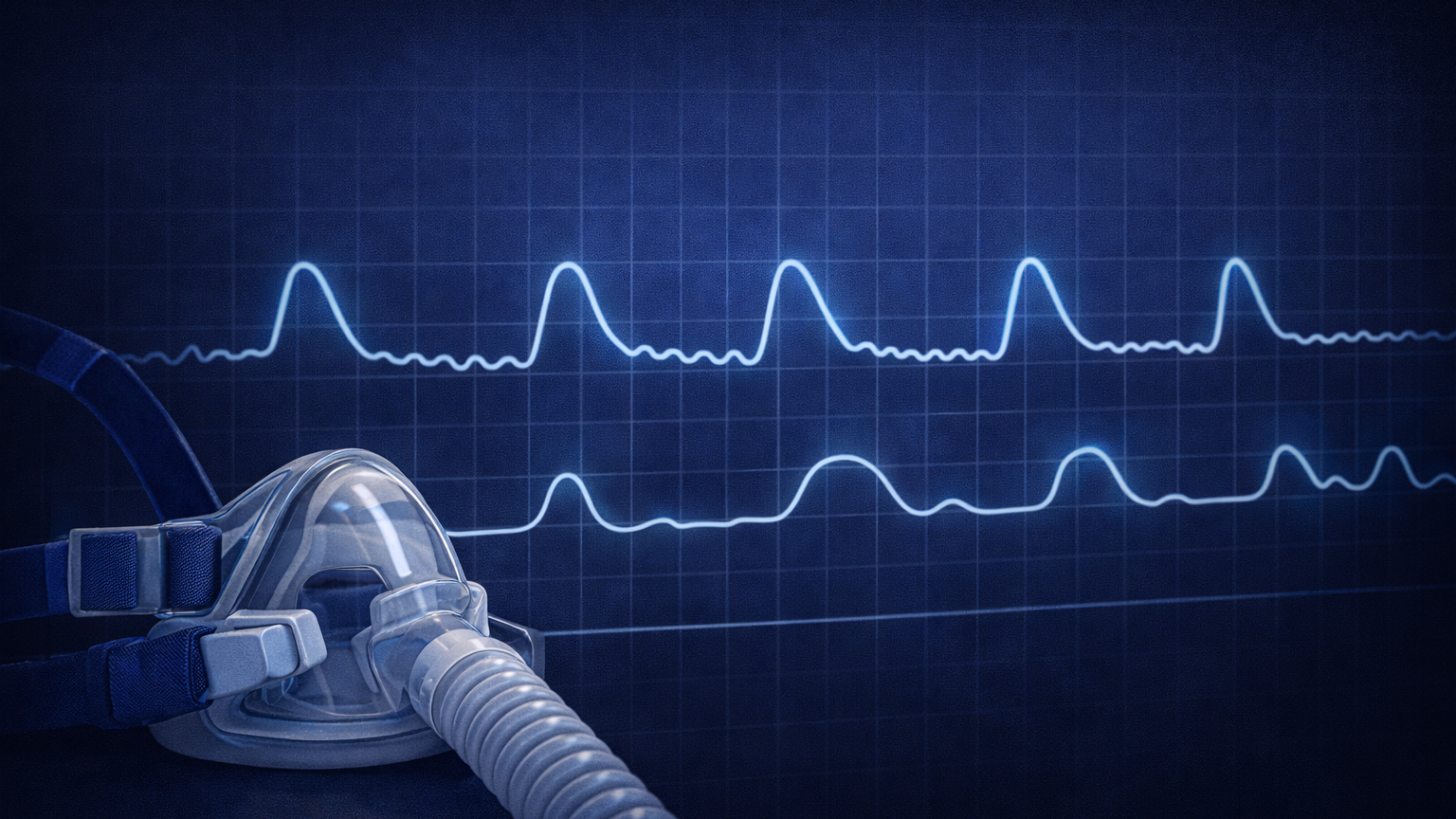
- Flow limitation trends
- Breathing waveform stability
- Sleep-stage continuity (when available)
- Oxygen variability
- Pressure responsiveness
- Night-to-night consistency
Individually, these metrics are complex. Together, they tell the real story.
Turning CPAP Data Into Insight (Not Guesswork)
Raw CPAP data is powerful—but overwhelming. Charts, graphs, and medical terms don’t automatically translate into actionable understanding.
This is where tools like SleepLink come in.
How SleepLink Helps
SleepLink analyzes your CPAP data holistically—not just AHI—to help you:
- Understand why you still feel tired
- Identify hidden breathing inefficiencies
- Spot trends that matter across nights
- Make informed, safe adjustments
- Have clearer, more productive discussions with clinicians
Instead of chasing a single number, you focus on sleep quality as a system.
The Bottom Line
AHI is a useful starting point—but it was never meant to define successful therapy on its own.
If you:
- Feel unrefreshed despite low AHI
- Suspect UARS or subtle breathing issues
- Want to understand your CPAP data at a deeper level
…it’s time to look beyond the headline number.
Better sleep comes from understanding the full picture—not just one metric.
Ready to See the Full Story?
Explore your CPAP data with clarity and confidence.
Try SleepLink at https://sleeplink.app and turn your CPAP data into meaningful insight.